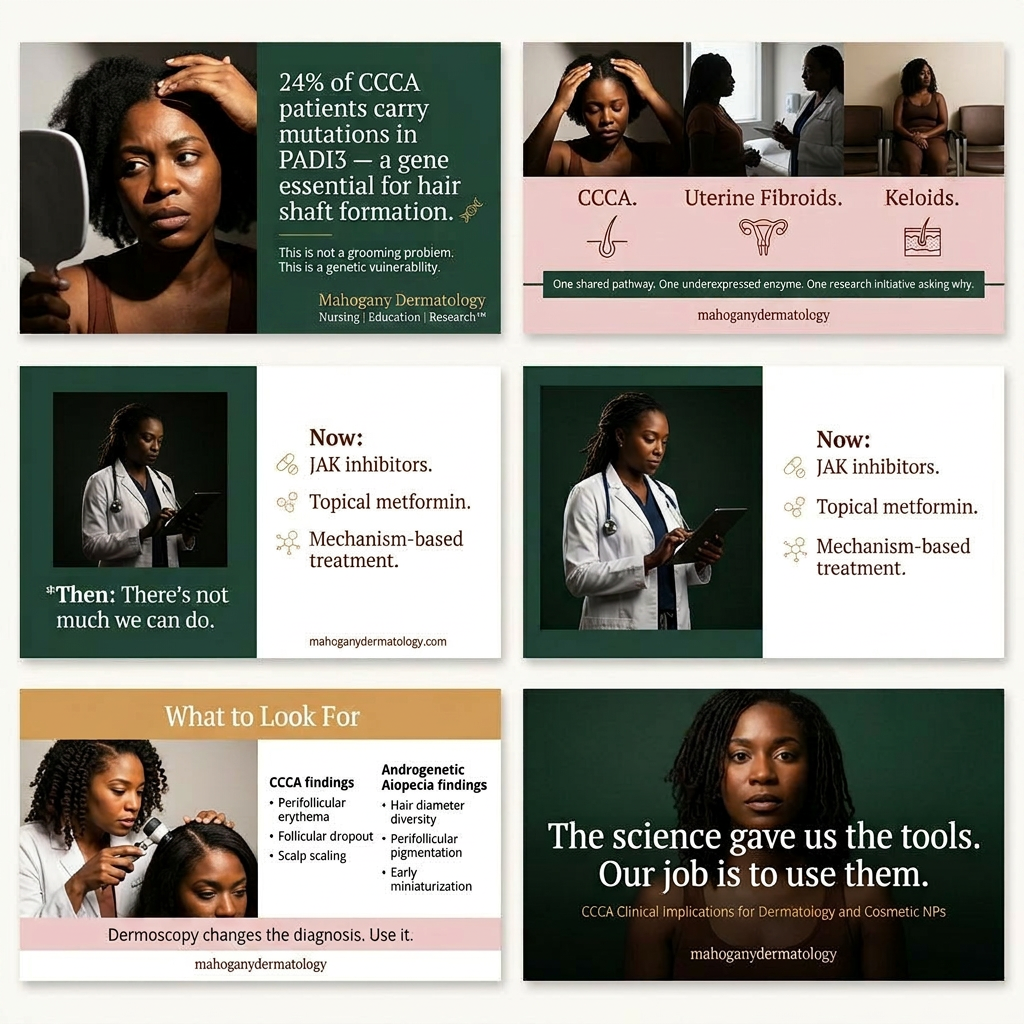
CCCA Is No Longer a "There's Not Much We Can Do" Diagnosis
The emerging science on CCCA has given us something we have never had before: a biological rationale for treatment decisions that go beyond symptom management. For the first time, we can point to specific molecular targets, prescribe mechanism-based therapies, and offer patients a realistic conversation about regrowth rather than just slowing loss. What the science cannot do is walk into a clinic room. That is our job. As dermatology and cosmetic nurse practitioners, you are not reading biopsies in isolation or running gene expression analyses in a lab. You are the clinicians sitting across from a Black woman in her thirties watching her hairline retreat, tracking disease progression month by month, managing expectations, and witnessing what permanent hair loss does to a person's sense of self. That continuity is not incidental to CCCA care. It is the mechanism by which the current evidence actually reaches patients. This article translates that evidence into clinical action. From closing the diagnostic gap that allows CCCA to be dismissed as androgenetic alopecia, to expanding the treatment conversation beyond corticosteroids, to navigating cost barriers and addressing hair care practices without blame, these are the implications that matter most for frontline NP practice.
This is a multiple-part series. Join the email list to be notified when each article is published:
+ Why We Are Investigating the Link Between Fibroids, Keloids, and Hair Loss (And Why We Need an Illustrator to Do It). Read here.
+ DNP and PhD Nurse Scientist Research Ideas. Read here.
+ Entrepreneurial Opportunities and Business Strategies. Read here.
Listen to audio version here.
Implications for Dermatology and Aesthetic Nurse Practitioners
As dermatology and cosmetic nurse practitioners, you occupy a unique position in the CCCA treatment landscape. You're not dermatopathologists reading biopsies in isolation from patients. We're not researchers running gene expression analyses in laboratories. You're the clinicians on the front lines, building relationships with patients over months and years, tracking disease progression, adjusting treatments, managing expectations, and witnessing the profound psychosocial impact of permanent hair loss.
This means we need to translate the emerging science into clinical action. Understanding that CCCA is a fibroproliferative disorder with genetic underpinnings doesn't just satisfy our intellectual curiosity, it fundamentally changes how we diagnose, monitor, and treat this condition.
First, we need to improve our diagnostic acumen. CCCA is underdiagnosed, often dismissed as androgenetic alopecia or attributed entirely to grooming trauma without proper investigation. When a Black woman in her thirties or forties presents with progressive vertex alopecia, CCCA should be high on your differential. Don't assume it's female pattern hair loss without examining for the characteristic signs: perifollicular erythema in early disease, the grayish perifollicular halos on dermoscopy, the centrifugal pattern of spread, the smooth scarred scalp in advanced cases.
Dermoscopy is invaluable here. In CCCA, you'll see decreased follicular ostia, absence of follicular openings in affected areas, perifollicular scaling, and polytrichia (multiple hair shafts emerging from a single follicular orifice). These findings differentiate CCCA from androgenetic alopecia, where you'd expect to see follicular miniaturization with preserved follicular openings and no scarring. If you're uncertain, biopsy. A 4mm punch biopsy submitted for horizontal sectioning can provide definitive histopathologic diagnosis and staging of disease severity.
Once diagnosed, we need to set realistic expectations with our patients while offering genuine hope. The traditional conversation about CCCA has been deeply discouraging: "This is permanent scarring alopecia. We can try to slow progression with steroids, but honestly, there's not much we can do. Consider a wig or surgical hair restoration." That's no longer accurate. We now have mechanism-based treatments showing real clinical benefit, including hair regrowth in patients with longstanding disease who'd failed multiple conventional therapies.
But regrowth takes time, months, not weeks, and not every patient responds to every treatment. We need to communicate that early intervention matters enormously. Follicles that have been completely replaced by fibrous tracts aren't coming back. But follicles that are inflamed, degenerating, or early in the fibrotic process? Those can be rescued with the right therapeutic approach. This is why leading dermatologists who specialize in hair loss for skin of color are aggressive about treatment in patients with active disease, even if the cosmetic concern seems minor at presentation.
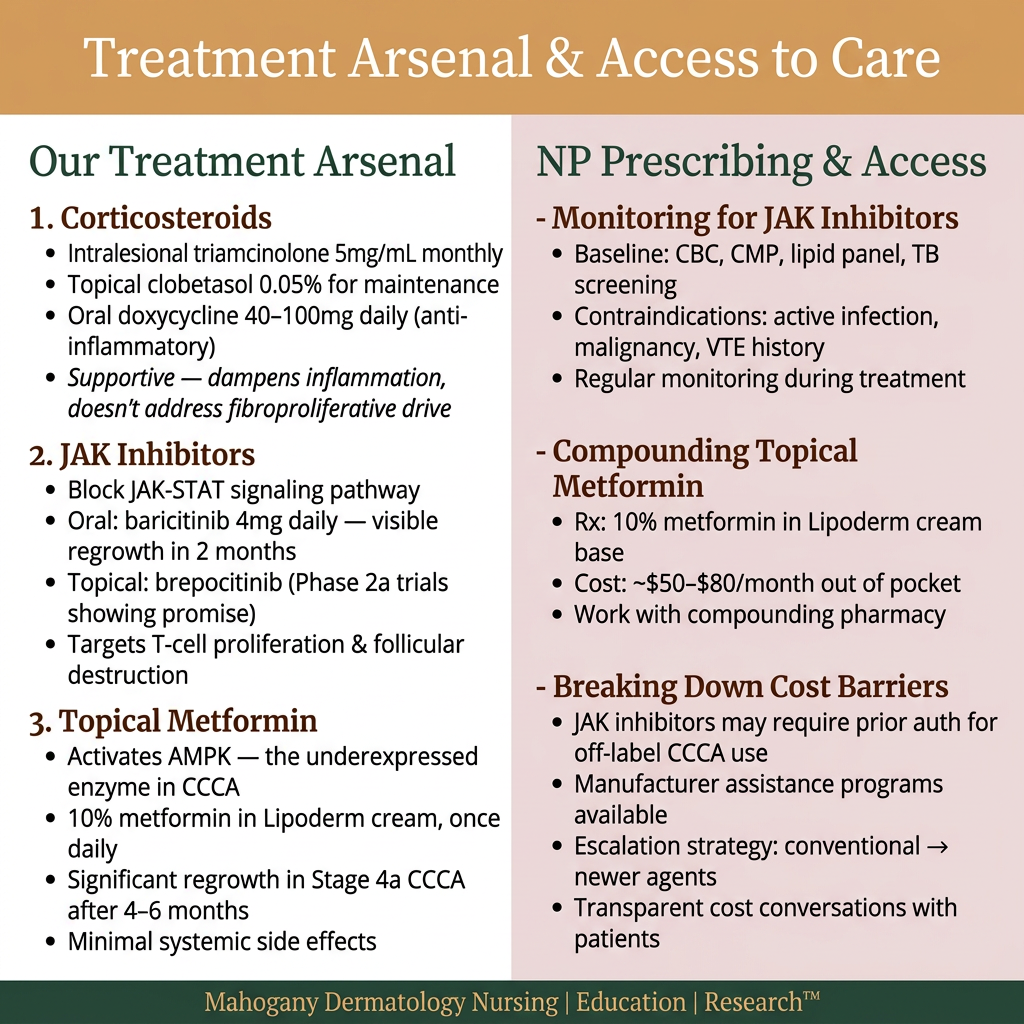
Steroids
Our treatment arsenal now extends beyond corticosteroids. Intralesional triamcinolone remains useful for controlling acute inflammatory flares, the latest research recommends 5mg/mL injections monthly to affected areas. Topical corticosteroids like clobetasol 0.05% ointment or solution can be used between injection appointments for maintenance. Oral doxycycline at 40-100mg daily provides anti-inflammatory benefit through non-antimicrobial mechanisms. But these are supportive therapies. They dampen inflammation but don't address the underlying fibroproliferative drive or genetic susceptibility.
JAK Inibitors
This is where the new therapeutic approaches come in. JAK inhibitors work by blocking the JAK-STAT signaling pathway that mediates inflammatory cytokine action. When activated, this pathway drives T-cell proliferation, inflammatory mediator production, and ultimately follicular destruction in CCCA. We've seen dramatic results with both oral JAK inhibitors like baricitinib and topical agents like brepocitinib in clinical trials and case reports. One patient treated with baricitinib 4mg daily showed visible hair regrowth after just two months, something we rarely see with conventional therapy. The brepocitinib Phase 2a trial in cicatricial alopecias is showing promising early signals of efficacy in CCCA patients.
Topical Metformin After Failing Conventional Therapies
Topical metformin represents another mechanism-based approach. Metformin activates AMPK, the very enzyme that's underexpressed in CCCA scalps. By restoring AMPK activity, metformin can reverse fibrotic processes, it's been shown to deactivate myofibroblasts and accelerate resolution of pulmonary fibrosis in animal models. When compounded at 10% in a cream base optimized for transcutaneous absorption and applied topically to CCCA scalps, metformin has produced substantial hair regrowth in patients who'd failed all conventional therapies. One case series reported two women with stage 4a CCCA showing significant regrowth after four to six months of daily topical metformin application. Neither experienced systemic side effects, though both reported scalp dryness that improved with moisturizer use.
As nurse practitioners, we can absolutely prescribe and manage these therapies. Topical metformin requires working with a compounding pharmacy, but the formulation is straightforward: 10% metformin in Lipoderm cream base, applied once daily to affected areas. For oral JAK inhibitors, we need to be aware of the monitoring requirements. Before starting baricitinib or tofacitinib, obtain baseline CBC, comprehensive metabolic panel, lipid panel, and tuberculosis screening. Monitor these parameters regularly during treatment. Screen for risk factors that would contraindicate JAK inhibitor use: active infection, malignancy, venous thromboembolism history, or significant immunosuppression.
Money Barriers to Care
Cost and insurance coverage are real barriers we need to navigate. JAK inhibitors approved for rheumatoid arthritis or alopecia areata may not be covered for off-label CCCA use. Compounded topical metformin typically costs patients $50-$80 monthly out of pocket. We need to have transparent conversations about cost and work with patients to find financially feasible approaches, whether that's starting with less expensive conventional therapies and escalating to newer agents if those fail, or helping patients access manufacturer assistance programs and copay support.
Cultural Sensitivity
We also need to address the hair grooming practices that may be triggering or exacerbating disease in genetically susceptible patients. But we need to do this with cultural sensitivity and without blame. Black women's hair care practices are deeply tied to cultural identity, professional presentation, and personal autonomy. Telling a patient to "stop wearing braids" without understanding the social, economic, and cultural context of that recommendation is both ineffective and damaging to the therapeutic relationship. Effective patient education focuses on the mechanical stress model: hair shafts may be more fragile due to genetic factors (PADI3 mutations), which means high-tension hairstyles, chemical relaxers, and thermal styling can trigger inflammation and progression in ways they wouldn't in someone without that genetic vulnerability.
The clinical conversation should explore what's most important to patients about their current hair care routine and what modifications they'd be willing to make. Potential harm reduction strategies include reducing braid tension, spacing out relaxer applications, incorporating more protective low-manipulation styles, or decreasing heat styling frequency. The goal is collaborative harm reduction, not prescriptive mandates about how patients "should" wear their hair.
Patient education extends to setting realistic timelines for improvement. With topical metformin or JAK inhibitors, patients may see decreased shedding and reduced symptoms within the first month, but visible hair regrowth typically takes four to six months of consistent use. I recommend photographing patients' scalps at each visit for objective monitoring; it's easy for both clinicians and patients to underestimate improvement when seeing each other regularly. Side-by-side photos taken three to six months apart often reveal progress that daily observation misses.
CCCA Is a Long Game
We also need to educate patients about the chronic nature of CCCA. This isn't like alopecia areata where treatment induces remission and you can stop therapy. CCCA requires long-term disease control. When we achieve stability or regrowth, we need maintenance therapy to sustain those gains. That might mean transitioning from intensive treatment with oral JAK inhibitors to maintenance with topical therapy, or continuing compounded metformin indefinitely. Discontinuing successful treatment often leads to disease recurrence, sometimes with rapid progression that erases months of gains.
For patients with extensive scarring who don't respond adequately to medical therapy, we need to discuss reconstructive options. Surgical hair restoration through follicular unit transplantation can be considered in patients with stable, inactive disease and adequate donor supply. Wigs, cranial prostheses, and micropigmentation offer non-surgical cosmetic solutions. But these discussions require sensitivity, many women feel they've "failed" if they need these interventions. Frame them as additional tools in the toolbox, not admissions of defeat.
From a practice management standpoint, treating CCCA requires time and continuity. These aren't fifteen-minute visits. Initial consultations need thirty to forty-five minutes for comprehensive history, examination, dermoscopy, discussion of diagnosis and treatment options, and expectation setting. Follow-up visits every six to eight weeks for reassessment and treatment adjustment work well for most patients. Building that continuity allows you to track subtle changes that indicate treatment response or progression.
Documentation is critical. Photograph affected areas at each visit, record extent of alopecia using the Central Hair Loss Grading scale, note any symptoms (itching, burning, tenderness), and document examination findings including signs of active inflammation versus burned-out scarring. This creates an objective record of disease activity and treatment response that's invaluable for adjusting therapy and demonstrating medical necessity to insurance companies.
Now It's Your Turn: Nursing Research
We also have a role in advancing CCCA research through practice-based data collection. Consider participating in patient registries, reporting cases of novel treatment responses to the literature, and collaborating with academic centers conducting clinical trials. CCCA has been neglected for too long. Those of you seeing these patients regularly can contribute to the evidence base that will guide the next generation of therapeutic advances.
Finally, we need to advocate for our patients at the systemic level. CCCA disproportionately affects a population that has historically experienced significant barriers to dermatologic care. We can advocate for research funding, insurance coverage of effective therapies, and training programs that ensure all dermatology providers can competently diagnose and manage hair disorders in patients of color. Every patient we educate, every case we document, every treatment success we share contributes to elevating CCCA from a neglected orphan disease to a condition with an established evidence-based treatment paradigm.
The science is giving us the tools. As nurse practitioners, our job is to translate that science into clinical practice that genuinely improves our patients' lives.
Survey Invitation: We invite you and your patients to participate in our preliminary data collection that is being used to inform the direction of our clinical research. Click here to take the survey.
About the Author
Dr. Kimberly Madison, DNP, AGPCNP-BC, WCC, is a Board-Certified, Doctorally-prepared Nurse Practitioner, educator, and author dedicated to advancing dermatology nursing education and research with an emphasis on skin of color. As the founder of Mahogany Dermatology Nursing | Education | Research™ and the Alliance of Cosmetic Nurse Practitioners™, she expands access to dermatology research, business acumen, and innovation while also leading professional groups and mentoring clinicians. Through her engaging and informative social media content and peer-reviewed research, Dr. Madison empowers nurses and healthcare professionals to excel in dermatology and improve patient care.
References
Araoye, E. F., Thomas, J. A. L., & Aguh, C. U. (2020). Hair regrowth in 2 patients with recalcitrant central centrifugal cicatricial alopecia after use of topical metformin. JAAD Case Reports, 6(2), 106–108. https://doi.org/10.1016/j.jdcr.2019.12.008
Heath, C. R. (2024). Part 1: Scalp and hair disorders in patients with skin of color [Presentation slides]. Dermatology Week APP Institute.
Lin, C. M. A., Cooles, F. A. H., & Isaacs, J. D. (2020). Basic mechanisms of JAK inhibition. Mediterranean Journal of Rheumatology, 31(Suppl 1), 100–104. https://doi.org/10.31138/mjr.31.1.100
Malki, L., Sarig, O., Romano, M. T., Méchin, M.-C., Peled, A., Pavlovsky, M., Warshauer, E., Samuelov, L., Uwakwe, L., Briskin, V., Mohamad, J., Gat, A., Isakov, O., Rabinowitz, T., Shomron, N., Adir, N., Simon, M., McMichael, A., Dlova, N. C., ... Sprecher, E. (2019). Variant PADI3 in central centrifugal cicatricial alopecia. New England Journal of Medicine, 380(9), 833–841. https://doi.org/10.1056/NEJMoa1816614
Ogunleye, T. A., McMichael, A., & Olsen, E. A. (2014). Central centrifugal cicatricial alopecia: What has been achieved, current clues for future research. Dermatologic Clinics, 32, 173–181. https://doi.org/10.1016/j.det.2013.12.005
Senna, M., Taylor, S., Piraccini, B., Shapiro, J., Somani, N., Jedynak, J., Ogwu, S., Buchanan, A., Craiglow, B., & Ohyama, M. (2024). Characterizing loss of response occurring in a small number of patients during 3 years of long-term maintenance therapy with baricitinib 4-mg: Results from BRAVE-AA1 and -AA2 trials [Poster presentation]. American Academy of Dermatology Annual Meeting. doi:10.25251/skin.9.supp.522
Workman, K., & Kindred, C. (2023). Hair regrowth in a patient with central centrifugal cicatricial alopecia after a 2-month trial of baricitinib. JAAD Case Reports, 39, 109–111. https://doi.org/10.1016/j.jdcr.2023.07.016
.svg)
.svg)
.svg)